






Patient Info
Diabetic Retinopathy
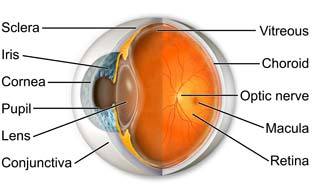
Diabetic retinopathy is the leading cause of acquired blindness among people under the age of 65. The great majority of this blindness can be prevented with proper examination and treatment by ophthalmologists (EyeMDs). An extraordinary amount of research has already been completed, and is relied upon heavily by practicing ophthalmologists, in the treatment of patients with diabetes. Unfortunately, patients who are not properly referred for evaluation and management or those who, for any reason, fail to get proper care from an ophthalmologist are at the greatest risk of vision loss. Ophthalmologists primarily rely on the results of four major clinical studies to guide their treatment of patients with diabetes mellitus. These are the Diabetes Control and Complications Trial (DCCT), the Diabetic Retinopathy Study (DRS), the Early Treatment Diabetic Retinopathy Study (ETDRS), and the Diabetic Retinopathy Vitrectomy Study (DRVS).
Background Diabetic Retinopathy
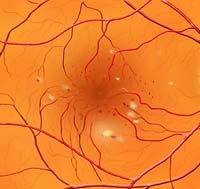
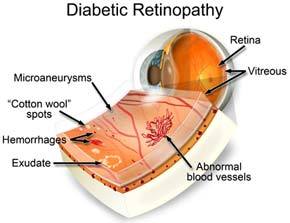
Background diabetic retinopathy (BDR) may occur at any point in time after the onset of diabetes. In general, this is the first “stage” of diabetic retinopathy and, therefore, the least concerning. This condition is often present without any visual symptoms. Findings in the retina include dot and blot haemorrhages (tiny haemorrhages in the retina itself), microaneurysms (out-pouchings of capillaries), and exudates (retinal deposits occurring as a result of leaky vessels).
The development of this condition in type I(juvenile-onset) diabetics is rare prior to three or four years following the onset of diabetes. In type II (adult-onset) diabetics, background diabetic retinopathy may be present at the time of diagnosis of the condition. Primary care practitioners should refer patients with diabetes to ophthalmologists, accordingly.
In general, patients with BDR do not need immediate treatment but assessment of the progress of the condition should be done annually. An exception exists for some patients with an advanced form of BDR known as pre-proliferative diabetic retinopathy. Ophthalmologists may recommend treatment at this stage, especially if the opposite eye has had diabetes related complications.
Clinically Significant Macular Oedema
Clinically significant macular oedema (CSME) is a condition of swelling of the macula related to the development of leaky capillaries and microaneurysms. This condition may or may not be associated with reduced or distorted vision. Ophthalmologists use rather strict criteria to determine whether a patient should be treated with focal laser photocoagulation for this condition. These criteria were set forth by the studies mentioned above.
Patients with CSME are generally recommended to undergo focal laser photocoagulation. This entails a fluorescein angiogram to guide treatment and utilisation of a laser to help “dry up” the localised swelling (macular oedema). Ophthalmologists apply laser treatment to the macula of the eye, avoiding the fovea where central acuity resides, in a grid-pattern or directly to leaking microaneurysms. The risk of visual loss is reduced by more than 50% for patients with CSME who undergo focal laser photocoagulation. Even patients with 20/20 vision who meet guidelines for treatment should be considered for laser therapy to prevent eventual visual loss. It is important to realise that laser treatment does not usually improve vision, but is aimed at prevention of further visual loss. Most patients with CSME require 3 to 4 different focal laser sessions, two to four months apart, to resolve the swelling.
In recent years, the use of anti-vascular endothelial growth factor (VEGF) has been a new treatment option for CSME. Several intravitreal medications are also available and pars plana vitrectomy procedure may also be performed. Pars plana vitrectomy involves removal of the vitreous or relieving vitreous traction which reduces macular oedema and improves vision.
Proliferative Diabetic Retinopathy
Proliferative diabetic retinopathy (PDR) carries the greatest risk of visual loss of the conditions discussed thus far. The condition is characterised by the development of neovascularisation (new, abnormal vessel growth) on or adjacent to the optic nerve and vitreous or pre-retinal haemorrhage (haemorrhage in the vitreous humor or in front of the retina). PDR usually occurs in eyes with advanced background diabetic retinopathy and is thought to be secondary to ischaemia (lack of oxygen or blood flow) of the retina. It has been theorised that a “neovascular growth factor,” acting as a local hormone, may cause the development of neovascularisation. Unfortunately, the neovascular vessels are abnormal and have a tendency to break and bleed into the vitreous humor of the eye. In addition to sudden vision loss, this may lead to more permanent complications, such as tractional retinal detachment and neovascular glaucoma.
Patients with PDR should receive scatter laser photocoagulation (laser treatment of the ischaemic peripheral retina) as soon as possible following diagnosis of the condition. This treatment is also known as pan-retinal laser photocoagulation. By causing regression of the neovascular tissues, the risk of severe vision loss is substantially reduced. Scatter laser photocoagulation (also known as PRP, or pan-retinal photocoagulation) is an in-office or out-patient procedure done with or without an anaesthetic injection adjacent to the eye. Many patients will experience mild discomfort with the laser treatment, although this can be resolved with an anaesthetic block. The laser treatment usually takes less than 30 to 45 minutes per session. A complete laser treatment, however, may require up to 3 or 4 different sessions, with a total of one to two thousand laser applications (“spots”).
In some patients with PDR, the vitreous haemorrhage prevents the ophthalmologist from performing the laser treatment. Simply put, the blood is in the way of the laser beam. If the vitreous haemorrhage fails to clear within a few weeks or months, a vitrectomy surgery may be performed to mechanically clear the haemorrhage and laser photocoagulation is then applied, either at the time of the vitrectomy or shortly thereafter. Patients who have tractional retinal detachment are usually scheduled for vitrectomy surgery promptly. In vitrectomy the vitreous gel clouded with blood is removed and replaced with salt solution. In certain cases with retinal detachment a gas bubble is also injected in the eye. The gas and the saline are slowly absorbed by the eye and the eye cavity gets replaced by the newly formed vitreous gel.
Both vitrectomy and laser treatment only prevent further deterioration of the disease condition in proliferative retinopathy but does not cure the disease. The problem may reappear and so regular follow up and regular comprehensive eye check up are very important in keeping the disease under control and preventing vision loss due to it.